

JOHN LI, M.D.
OTOLOGY NEUROTOLOGY RESOURCES
210 Jupiter Lakes Blvd #5105
Jupiter, FL 33458
Phone: (561)-748-4445
Fax: (561)-748-4449
Superior Canal Dehiscence
Superior Canal Dehiscence Surgery More Info Link
This a transcript of my Powerpoint Slide Lecture given to a PA Academy conference:
History
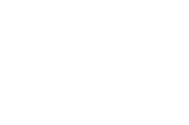
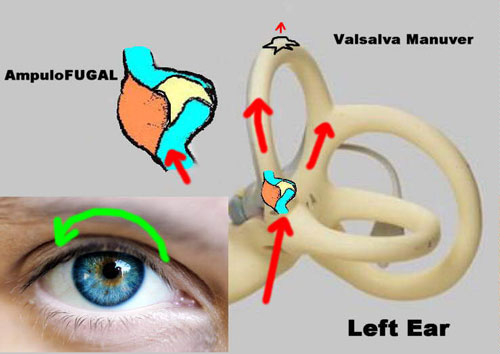
Diagrams of the Valsalva Maneuver
1929 Tullio first described sound-induced nystagmus in pigeons eye movements in response to loud noises - Tullio’s phenomenon.
1911 Hennebert: eye movements evoked with pressure in the external auditory canals in congenital syphilis patients
Nadol: speculated re: adhesions between the foot plate and saccule
1998 Dr. Minor: described superior canal dehiscence syndrome.
The Typical Signs
Vertigo and oscillopsia evoked by sounds.
Sound induced vertigo occurs in about 97%
Activities that change middle ear intracranial pressure cause vertigo in approximately 82% of patients.
Chronic disequilibrium
Hyperacusis was found at 39% of patients
Evoked Nystagmus
Eye movements in the plane of the superior canal evoked by sounds in 89%
Evoked by valsalva maneuvers in 82%
Tragal pressure in 54%.
21% of patients showed head movements evoked by sounds.
Sensitivity to Bone Conduction
Hearing their joints moving,
Hearing their eye movements
Hearing their heart beat
Hearing their heels strike during walking
Hear a tuning fork placed at a distal extremity.
Physical Examination
Spontaneous nystagmus is generally not appreciated. Subtle evoked nystagmus is common
Use frenzel or IRV goggles
Pneumatic otoscopy and valsalva maneuvers may produce the nystagmus.
Weber: is usually to the affected side
Rinne: tuning fork test: BC >AC
Hear a tuning fork placed on the extremity
Objective Evaluations Include
VEMP
Radiology
Vestibular-Evoked Myogenic Potential Testing (VEMP)
Based on the fact that the saccule is actually sensitive to sound
Useful for detecting abnormal sensitivity to otoliths to sound.
Equipment:
Evoked response computer
Sound generator
Surface electrodes to pick up neck muscle activation
Short latency relaxation potentials in the sternocleidomastoid muscle.
Audiologic Findings
Decreased bone conduction threshold.
Conductive hearing loss: due to dissipation of sound energy due to the third window effect.
Intact acoustic reflexes could help differentiate otosclerosis from superior canal dehiscence syndrome.
Treatment
Varies in corresponding to the severity of symptoms
Education
Identify and avoid aggravating factors -- might be able to avoid surgery
Pressure equalization tube may relieve symptoms of disequilibrium and unsteadiness, especially in patients with concurrent eustachian tube dysfunction.
Surgical Treatment
Superior Canal Resurfacing vs. Canal plugging (as in cases of intractable benign positional vertigo.)
Middle cranial fossa approach vs. Transmastoid approach
Possible loss of vestibular function
Possible sensorineural hearing loss
A plug composed of fascia and bone dust
Superior Canal Resurfacing
Preserves the physiologic function of the semicircular canal
Fascia is placed over the dehiscence
Tucked under the edge of the bone
Bone graft
Fascia again
Fibrin glue
Potential Pitfalls
This technique may also result in vestibular hypofunction.
Bone graft may resorb with time.
Fascia or the bone graft could slip out of place
Return of symptoms
Conclusion
Superior canal dehiscence syndrome is characterized by pressure and/or sound-induced vertigo.
Physical exam findings include pressure-induced nystagmus, localization of Weber tuning fork test and vertigo with sound.
This entity is diagnosed with clinical findings and confirmed by CT scan or other objective testing.