

JOHN LI, M.D.
OTOLOGY NEUROTOLOGY RESOURCES
210 Jupiter Lakes Blvd #5105
Jupiter, FL 33458
Phone: (561)-748-4445
Fax: (561)-748-4449
BPPV Canalith Repositioning The 360 Maneuver & Repositioning Chair Surgery for BPPV Posterior Canal Occlusion
Posterior Semicircular Canal Occlusion
 Surgery is usually reserved for cases that fail standard canalith repositioning procedures. There are several surgical options. Labyrinthectomy of the affected ear can be quite effective for benign positional vertigo. However, it seems to be too aggressive for the type of pathology involved. Historically, singular nerve section, was reportedly the treatment of choice. However, few if any surgeons were able to accomplish this procedure successfully without damaging vital hearing structures. Transtympanic application of aminoglycosides (such as Gentamicin and Streptomycin) is also an option. However, like labyrinthectomy, it may be overkill.
Surgery is usually reserved for cases that fail standard canalith repositioning procedures. There are several surgical options. Labyrinthectomy of the affected ear can be quite effective for benign positional vertigo. However, it seems to be too aggressive for the type of pathology involved. Historically, singular nerve section, was reportedly the treatment of choice. However, few if any surgeons were able to accomplish this procedure successfully without damaging vital hearing structures. Transtympanic application of aminoglycosides (such as Gentamicin and Streptomycin) is also an option. However, like labyrinthectomy, it may be overkill.
Each person has six semicircular canals (three on each side) and four linear acceleration sensors. Labyrinthectomy and transtympanic application of aminoglycosides destroys three of the semicircular canals and two of the linear acceleration sensors (very destructive). Since Posterior Semicircular Canal Occlusion only treats the one affected semicircular canal from benign positional vertigo, it is considered the least destructive of the surgical treatment options.
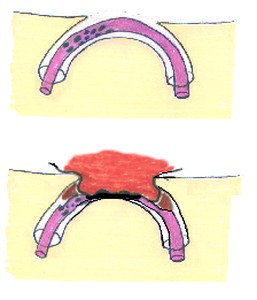
The idea behind semicircular canal occlusion is based on the fact that the vertigo is caused by movement of particles within one of the semicircular canals. Crushing the canal would obviously immobilize these particles and thus stop the vertigo.
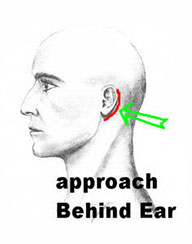
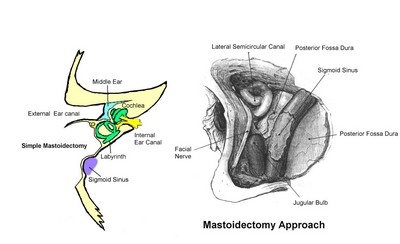
Canal occlusion is performed by working through a mastoidectomy approach. The affected semicircular canal needs to be positively identified with preoperative testing. The identified canal is then surgically outlined with a fine diamond drill bit. The membranes within the semicircular canal are delicately handled to avoid complete fluid leakage. The membranes are then occluded with muscle and autologous tissue grafting, trapping and immobilizing the particles.
Posterior semicircular canal occlusion is perhaps 95 percent effective in those who fail standard canalith repositioning procedures. The risks and complications include bleeding, infection, dizziness, imbalance, facial nerve damage, hearing loss, tinnitus, and anesthetic complications. Typically, patients do fairly well in terms of vertigo control. Sometimes they have little bit of residual imbalance because of the lack of proper impulses from the abolished semicircular canal. This imbalance usually improves with some balance re-training. There is perhaps a 5 to 10 percent chance of a minor hearing loss. There is typically less than 3 percent chance of total hearing loss in the affected ear.
Sometimes a course of vestibular rehabilitation is useful in compensating for the lack of the abolished semicircular canal.
Related Pages
BPPV Canalith Repositioning The 360 Maneuver & Repositioning Chair Surgery for BPPV Posterior Canal Occlusion
External Articles, authored by Dr. Li in E-Medicine Online and Medscape
Medscape: BPPV Medscape: BPPV Clinical Presentation ENT Today: BPPV Diagnosis and Treatment